
A C-section is a real operation and not bloodless
So what's a nephrologist doing writing about an Ob-Gyn topic? Well, to begin with I've delivered fifty babies, just none recently, so I've always had an Obstetrics interest. I was reading the latest edition of JAMA and saw an article in the "Clinical Crossroads" section titled "Elective Cesarean Delivery on Maternal Request." That caught my attention so I started reading about C-sections versus vaginal deliveries. The CDC webpage on the subject said in 2010 there were 1,309, 182 C-section deliveries in the US versus 2,680,947 vaginal deliveries. So nearly a third of all American deliveries were via C-section.
That hasn't changed significantly in the last few years; there's a 2007 article "Recent trends in Cesarean Delivery in the United States" which documents the increase in the percentage of deliveries done by C-Section rising from 21% in 1994 to 26% in 2002, 30% in 2005 to the plateau from 2007 through the most recent data I could find, a mid-June 2012 report in the publication, Healthgrades.
The 2007 report has details on C-section rates versus age of the mother and, as I expected, the percentage of deliveries done by this method rises steadily as the mom's age does. For those under age 20, the rate was 23%, for women over 40 it rose to 48%. All racial and ethnic groups experienced a similar increase from 1996 to 2007 and excluding American Indian and Alaskan Native women, all the other groups had C-section rates of 30% or higher.
State by state differences were considerable with four (Alaska, Idaho, New Mexico and Utah) staying under 25% and five others (Florida, Louisiana, Mississippi, New Jersey and West Virginia) topping the list at over 35%.
A 2010 paper from the World Health Organization looked at Cesarean rates in 134 countries. There were 54 in which the rate was less than 10%, 69 where it was greater than 15% and only 14 in the 10-15% zone WHO considered optimal.
That's amazing when we consider the WHO figure versus those in the United States. In 2006 a C-section was the most frequently performed surgery in U.S. hospitals!
There are a host of recognized medical indications for doing a C-section, those may include a fetus in an unusual position (not head-down), a maternal condition that may be worsened by labor (e.g., heart disease), an unusually large baby, a fetus with a known health problem, maternal infection with genital herpes or HIV, some multiple pregnancies (conjoined twins, AKA Siamese twins) or a placenta that is blocking the cervix (placenta previa).
Beyond clinical reasons for having this surgical procedure, there's maternal preference. The JAMA article was part of a series called "Conferences with Patients and Doctors," and presents the case of a late 30s primip (woman having her first baby; technically it should mean one who has already had a baby) who requested a C-section; she happens to have worked since she was twenty as a paralegal in a firm that handles mostly medical malpractice claims, so her viewpoint is very likely to be skewed.
The term itself, cesarean delivery on maternal request, with its acronym CDMR, sprang from an NIH State-of-Science-Conference Statement dated March 27, 2006. An 18-member panel reviewed the pertinent literature and heard comments for 18 experts in appropriate fields. They concluded there was not sufficient evidence to fully evaluate the pros and cons of CDMR versus vaginal delivery, but noted that the incidence of C-section without medical or obstetrical indications was increasing in the U.S.
At that time the authors thought a decision for CDMR had to be individualized and ethical principles must be adhered to. They also noted that CDMR should not be recommended for women who planned to have more than one child as there were increasing risks in each subsequent cesarean delivery.
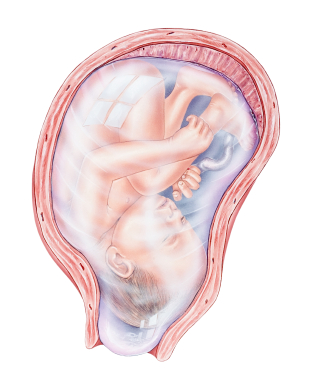
The placenta is the thickened area on the top of the uterus
What are those risks? Besides a difficult C-section in subsequent deliveries, sometimes leading to hysterectomy, need for blood transfusion or other surgical complications, there are potential problems with the mother's womb. The placenta, the structure that develops in the uterus during pregnancy to provide oxygen and nutrients to the fetus and remove its waste products, normally attaches to the lining of the uterus on the top or side of that organ.
A variety of issues can affect the placenta: increased maternal age is associated with a number of those as are high blood pressure, blood-clotting disorders, substance abuse or abdominal trauma.
Two placental abnormalities are more common with repeated C-sections and, in turn, may necessitate another Cesarean delivery or even a hysterectomy. Placenta previa means the structure has partially or even totally covered the cervix, instead of attaching to the top or side of the womb. This condition can lead to severe vaginal bleeding either prior to or at the time of delivery. The likelihood of placenta accreta also increases when placenta previa is present, especially when the mother has had repeated C-sections.
Normally the attachment of the placenta to the uterus, via small blood vessels termed chorionic villi, is relatively superficial, allowing easy separation of the structure after the baby is delivered. In placenta accrete, the viili penetrate deeper into the wall of the uterus, into a muscular layer called the myometrium.
When this happens, vaginal bleeding can happen during the third trimester of pregnancy, heavy bleeding can occur after the baby is delivered, the placenta can fail to separate from the uterine wall after the delivery and a C-section and surgical removal of the uterus may be required. The risk of placenta accreta is increased in areas of uterine scarring, often caused by a prior C-section.
The NIH Consensus Conference on the subject and the American Congress of Obstetricians and Gynecologists (ACOG) issued three recommendations for planning CDMR: It should not be done before a gestational age of 39 weeks has been accurately determined (allowing the fetus to have adequate lung development); It shouldn't be motivated because of fear of inadequate pain management, and It should not be recommended for women who wish to have several more children.
ACOG and medical ethicists feel that women need to have informed discussions of these issues, but, in the end, the obstetrician can ethically agree to a C-section. They are not required to do one and if the patient and her physician cannot agree on the route of delivery, it is appropriate for the doctor to refer her to another obstetrician.
