My own eye history is complex: I found out I was nearsighted at age eight while attending a baseball game with my folks. They mentioned the score and I asked how they knew what it was.
"Just read the scoreboard," Dad said.

My eyesight isn't perfect, but I haven't gotten to this stage yet
"What scoreboard?"
Much later, after years of wearing glasses (now they're bifocals), I was diagnosed as having a corneal disease...and that was even more years before the cataracts.
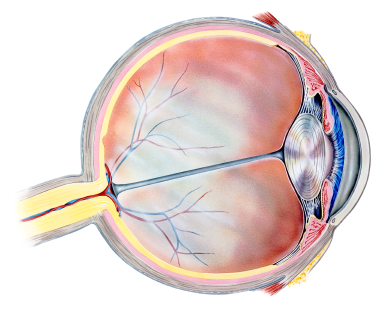
In my last post I outlined the anatomy and physiology of vision so that I could focus (pun intended) on diseases of the cornea and also on age-related macular degeneration this time.
In my prior post on the eye, I translated dystrophy as "it grew incorrectly," but "dys" comes from the Latin for "bad" and "trohe" from the Greek for "food," so poorly or inadequately nourished perhaps would be a better rendering for the term. A National Eye Institute document I provided a link to previously, "Facts about the Cornea and Corneal Diseases," says all of these dystrophies share a number of traits. They are usually inherited, affect both eyes equally, aren't caused by diet or injury, progress gradually and aren't related to systemic diseases, those that affect the rest of the body. They define a corneal dystrophy as "a condition in which one or more parts of the cornea lose their normal clarity due to a buildup of cloudy material."
Let's start with keratoconus, an abnormality of the cornea that usually affects both eyes, most frequently occurs in those who are ages 10 to 25 and slowly progresses over roughly a decade. It results in thinning and bulging of the cornea which forms a cone shape. This is a relatively uncommon disease affecting one in 2,000 of us and in its early stages can often be corrected with glasses or soft contact lenses.
Later on other kinds of contacts or even corneal transplantation may be required. If the patent gets such a transplant, its success rate is quite high with one estimate of an 89% positive outcome lasting ten or more years. An experimental treatment called collagen cross-linking is being evaluated around the world with clinical trials in multiple centers in the United States.
Less than 10% of those who have keratoconus also have a family history of the disease. Others may have had an eye injury, have other eye diseases, or unlike most other corneal problems, their keratoconus may be associated with systemic disorders including Down Syndrome.
My mother was said to have Fuchs' dystrophy, a slowly progressive corneal problem that normally affects both eyes, rarely alters vision until those who have it are in their 50s and 60s, and causes early-morning blurring that gradually clears as the day progresses. One layer of cells in the cornea, for unknown reasons, slowly dies off. They normally help pump water out of structure and, in their absence, the cornea swells, distorting vision.
Fuchs' is a major problem and some affected by this disease require advanced treatments including corneal transplantation. The success rate for this is reasonably good (73% after ten years), but waiting for donor tissue to become available is an issue.
I have map-dot-fingerprint (MDFD) dystrophy, according to most sources the most common of over 20 conditions in which parts of the cornea lose their usual clearness as cloudy materials pile up.
MDFD usually hits adults between the ages of 40 and 70, but can develop earlier. I remember cutting my right eye with a paper towel in 1971 when I was 30. It healed slowly and I had recurring episodes of eye pain, especially when I first woke up, over a period of four or five months. I'd bet that was my first hint of MDFD which typically will have flares over a few years and then go away without any long-last effect on vision.
A 2012 Medscape article says MDFD is rarely hereditary and may better be described as a corneal degeneration. Estimates of its prevalence in the general population range widely, from 2 to 43%. Like me, up to a third of those with MDFD have repeated early morning corneal tears/rips termed corneal erosions. They happen because in MDFD the outermost of the cornea's five layers of tissue, the epithelium, doesn't stay correctly attached to the layer below.
Since your eyes naturally get dry at night, your eyelid may stick to the epithelium and when you first awake and open your eyes, the not-well-attached epithelium can tear off casing mild to even severe pain.
I'm going to move to the back of the eye and age-related macular degeneration (AMD). Remember that light from images we see passes through the lens and goes to the retina, a light-sensitive layer of cells that line the inner surface of the eye. As the light impinges on these cells, two types of them react to the stimulus with a series of chemical/electrical events that eventually trigger nerve impulses sent through the optic nerve to the visual centers of the brain. One kind is called rods and they are most important in dim light and provide our black and white vision. The other kind are termed cones and those are useful in our color perception and in daytime vision. I'll ignore a third type of receptor cells, important in reflexive responses to bright daylight.
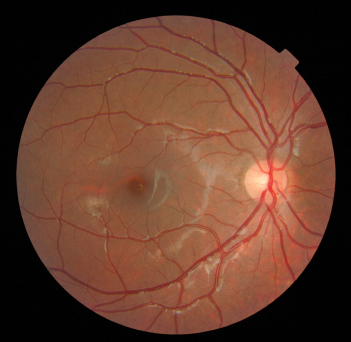
The macula is the dull round area slightly off-center
Near the center of a retina is a small, oval-shaped spot called the macula (Latin for "spot") that is critical for high-resolution vision. It's yellow in color, absorbs UV and blue light and is sometimes referred to as a natural sunblock protecting this highly-important area of the retina. The yellow color comes from two chemicals, lutein and zeaxanthin, which are derived from our diet. They are members of the carotenoids, a group of greater than 700 fat-soluble nutrients that provide the color in foods like carrots, pumpkins, sweet potatoes and other yellow, red, orange and deep green fruits and vegetables. Some of these, but by no means all, are converted to vitamin A or retinol, its active form, in the body.
AMD is the leading cause of major loss of vision in those of us over 50, accounting for more than half of all blindness in the United States. A major project, The Age-related Eye Disease Study (AREDS) has shown that taking some supplements can reduce the risk of progression to advanced AMD by 25% at 5 years. I've been taking a half dose of one of these for some years. Now a recent article in JAMA, "Lutein +Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration, part of the followup study, AREDS2, looked at specific components of those formulations of antioxidant vitamins and minerals.
Their conclusion was adding the two carotenoids, lutein and zeaxanthin (L&Z), and the omega-3s to the basic ingredients didn't seem to offer a further reduction in risk of AMD, but L&Z might lower the risk of lung cancer in former smokers.
I'm not changing the pill I now take. I don't think ingesting the equivalent of a little extra carrot or sweet potato will hurt me.